
Mesh Complications Patient Story 58
Lower Abdominal Pain, Pain Upon Sitting, Vaginal Pain, & Mesh Erosion into Rectum
Mesh Complications: Pain with sitting, lower abdominal pain and after rectal exams. Pain with defecation and pain in vagina.
Treatment: Posterior and Anterior repair and rectal wall mesh removal
The patient is a 56-year-old female from Chattanooga, TN with mesh erosion in the rectum. She reports pain upon sitting, after rectal exams, pain in her lower abdomen and the vagina. The patient had surgery four years ago and at that time had both Anterior & Posterior Prolifts (treatment of cystocele and rectocele using mesh) and a TVT Secure sling for cough urine leakage. She reports she felt well for several years then she began having pain. A colonoscopy done three years later revealed mesh in the rectum (Figure 1). She does admit to pain with intercourse but has had intercourse rarely.
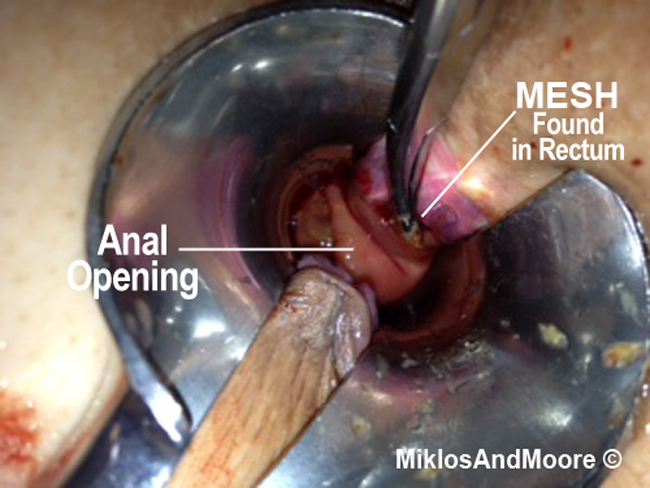
Figure 1
She came to see Drs. Miklos & Moore for evaluation and surgery. On exam, palpation of the edges of the bladder mesh (i.e. Anterior Prolift) and the rectal mesh (Posterior Prolift) recreated severe pain. The anterior mesh was not evenly distributed as if it dislodged after the initial surgery. Rectal exam confirmed mesh in the rectum and severe pain. Also noted the patient still had a cystocele, rectocele, and vaginal vault prolapse. Both the cystocele and rectocele were grade two.
Dr. Miklos Note: Despite having an Anterior and Posterior Prolift the patient still has both a cystocele and a rectocele. It is possible that surgeries fail. Unfortunately, this patient is not only suffering with pain, but she still has a rectal and bladder prolapse. This patient not only needs the Prolift removed from both the anterior and posterior aspect of the vagina because of pain, but the mesh is in the rectum and needs removal.
Surgery: The posterior vaginal wall was opened and the most distal portion of the mesh was identified and the vaginal skin was dissected away from the underlying mesh (Figure 2).
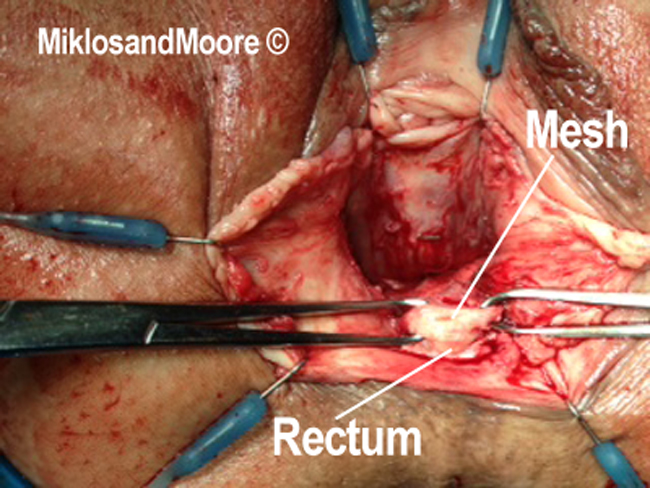
Figure 2
The dissection was extended up to the mesh, which was through the rectal wall. Note the finger in the rectum pushing up on the mesh. Further dissection of the mesh allows for the mesh to be dissected out of the rectal wall. Note the fingertip coming up through the hole in the rectum and floor of the vagina (Figure 3 & 4).
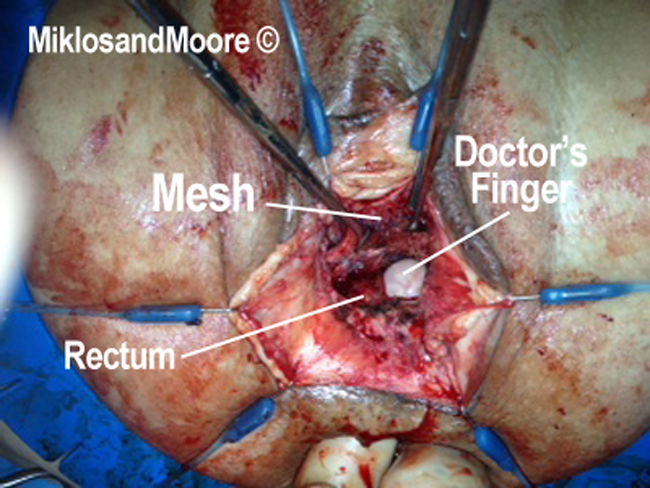
Figure 3

Figure 4
The very deepest portion of the mesh was identified using a right angle dissector. Two clamps were used to pull toward the surgeon and the right angle clamp identifies the deepest portion. The whole length of the mesh has been dissected and detached measuring approximately six centimeters (Figure 5).
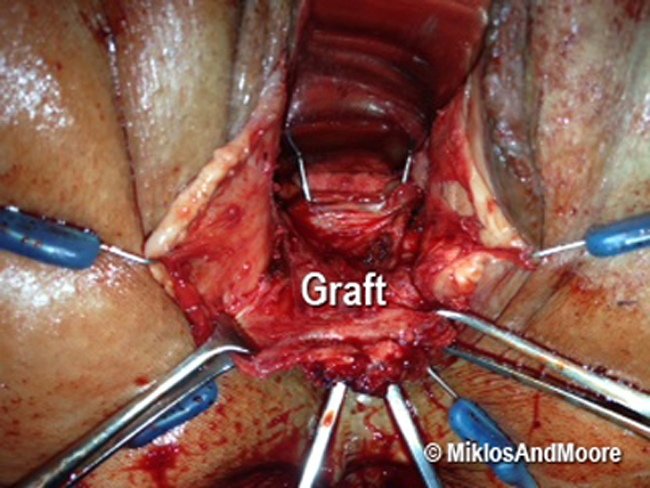
Figure 5
Once the mesh was completely removed our full attention was on repairing the hole in the rectum. The first layer of repair used nine individual sutures (Figure 6).
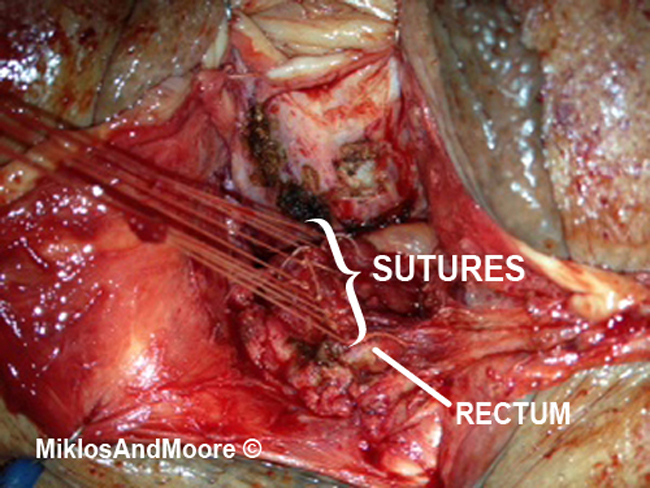
Figure 6
The removed mesh is seen (Figure 7).

Figure 7
The patient has had her mesh removed and continues to recover. She believes some, but not all of her pain is been alleviated. She is to undergo physical therapy to deal with post surgical pain.